|
Medical-Legal Illustrations, Animations and Interactive Media: Personal Injury Lawyers' Perceptions of Effective Attributes |
| Stephen R. Mader B.Sc., B.Sc.AAM,
M.Sc.BMC, CMI A literature review identified a lack of research on effective attributes of medical-legal illustrations, animations and interactive media. In this study, 20 personal injury plaintiff lawyers practicing in Southern Ontario, Canada, were surveyed about their perceptions of medical-legal visuals created for a hypothetical case involving a cervical fracture dislocation. Characteristics identified as most important included those that made the visuals comprehensible, personalized, credible and admissible. Respondents expressed an interest in depicting the entire injury sequence from trauma to long-term complications, including the injury mechanism. The survey group also indicated an interest in interactive user-controlled media. From these responses, recommended guidelines for creating effective medical-legal visuals were developed.
|
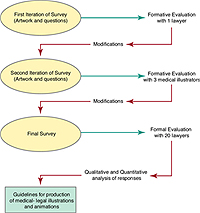
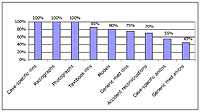
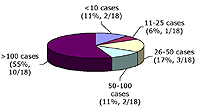
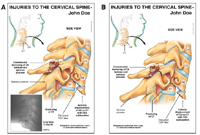
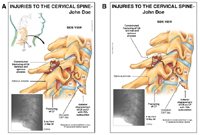
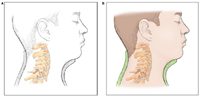
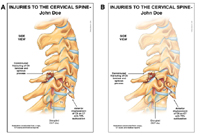
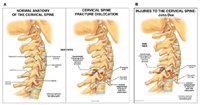
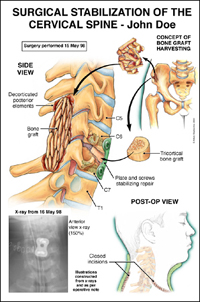
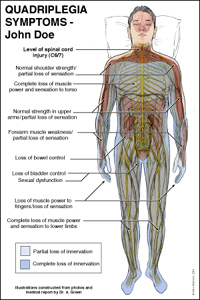
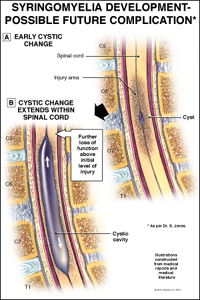
IntroductionDemonstrative evidence has become prevalent, indeed, essential for use in personal injury litigation (Turbak et al 1994). Visual presentations communicate more information with more emotional impact at a faster rate than oral descriptions (Simmons and Lounsbery 1994; Jew and Peterson 1995), and are more compelling, memorable, objective and succinct than lecture-format legal arguments (Turbak et al 1994). These visuals help medical experts clearly communicate complex facts to a jury and other trial participants, increasing understanding and retention of important issues throughout the course of a medical-legal trial (Mader 2003). Visual aids simplify complex facts without compromising accuracy (Turbak et al 1994). They focus on the critical issues in an appealing manner and provide a concise, yet comprehensive story (Babcock and Bloom 2001). Moreover, these visuals may be created in different media to repeat key pieces of evidence without the appearance of repetition, thus promoting the retention of critical information (Oatley 2000). Historically, medical-legal illustrators such as Jack Diner, Joan Beck and Dorothy Irwin provided guidance for the conceptualization and production process for medical-legal illustration panels (Diner 1963, Beck 1984, Irwin 1987). However, these guidelines were written before computers became ubiquitous and before the regular production of animation or interactive media for use in legal proceedings, as is common today. Despite plaintiff lawyers’ widespread use of medical illustrations during settlement negotiations (e.g., mediation) and trial, only minimal research has been done to determine which types of visual materials are most effective, that is, which are most didactic and most persuasive when presented to a jury, judge, opposing counsel or any other participants in the legal process. Turbak et al (1994) assert that these visual aids must be simple, focused and accurate, but a thorough search of the literature revealed that no study has actually tested this claim and published the findings. Feigenson and Dunn (2003) point out that despite the common use and admission into evidence of computer-generated animated reconstructions, the literature contains very few studies about how animations affect legal decisions. They propose a framework for testing several forms of visuals, starting with the basics (e.g., color) and advancing to an examination of the persuasiveness of case-specific prototypes related to advocates’ case theories. Some research has been conducted to examine ways in which mock jurors perceive demonstrative evidence and make decisions. Douglas et al (1997) examined the influence of photographs on judgments, and Kassin and Dunn (1997) looked at the effect of computer-generated animations on mock jurors’ decisions. Mock jurors' testing of demonstrative evidence has come under criticism. Diamond (1997) identifies common problems with jury simulations, including inadequate stratification sampling (most often using students), trial simulations (using only a short précis of a long trial), lack of jury deliberations, and the potentially distorting effect of mock juror role-playing on research findings. Personal injury lawyers, conversely, have firsthand experience of the response of actual jurors when an illustration or motion media is used in the courtroom. They present medical illustrations during trial in conjunction with the testimony of their medical experts (Oatley 2000) to explain complex medical concepts to the jury, including the significance of the injuries sustained by the plaintiff. With this experience, trial lawyers understand the psychological impact that visuals have on jurors (Oatley and McLeish 2004). In Canada, mediation may be arranged by plaintiff and defense counsel before trial, with a professional mediator present to facilitate resolution (Wheatley 2004). Unlike at trial, however, there are no evidentiary rules during this form of settlement negotiation. The demonstrative evidence used in this setting must focus on the main issues and be designed to educate the other side about complex issues (Wheatley 2004). At mediation, lawyers may present the visuals differently than they do during a trial. PowerPoint™ presentations with embedded medical illustrations and motion media (Mader 2003) may be used. During this type of case presentation, opposing counsel assesses the credibility of the case and the litigants to determine what impression may be made on the judge or jury (Wheatley 2004). Although the vast majority of cases settle before trial, the lawyer should approach a file as though it will proceed to trial and prepare accordingly (McLeish 2004). Consequently, use of medical illustrations at the settlement-discussion stage demonstrates a complete, trial-ready case and may increase the psychological edge during mediation (Mader 1995; Oliver 1994). When presenting visuals at mediation, the plaintiff’s lawyer understands how the jury may react to the illustrations should the case proceed to court (Oatley and McLeish 2004) and communicates this to defense counsel and adjusters. An analysis of the literature revealed that personal injury plaintiff lawyers have not been formally surveyed to gather their opinions and observations about what kinds of demonstrative evidence are the most effective at mediation or trial. These lawyers, nevertheless, because of their direct experience, are well-positioned to gauge how defense counsel, adjusters, judge and jury will respond to the medical-legal visuals that they present. Criteria for effective visuals used during legal proceedings could help medical illustrators create these visuals and, at the same time, may help personal injury plaintiff lawyers successfully settle cases before they proceed to trial. For those cases that go to trial, using the most effective visuals may speed the process, thus making more efficient use of court resources (Mader 2003). Despite the important role that medical-legal visuals play in personal injury litigation, there is a paucity of published research on their use. The purpose of this study was to determine which characteristics of medical-legal illustrations or motion media are effective, according to the perceptions and preferences of personal injury lawyers, and to delineate a set of guidelines based on the research results. Methods OVERVIEW OF EVALUATION METHOD This research project was structured as an expertise-based evaluation (Worthen and Sanders 1987). Twenty personal injury lawyers from Southern Ontario, Canada, were surveyed about their preferences and perceptions of the important attributes of effective medical-legal visuals for a hypothetical case involving a cervical fracture dislocation. A number of illustrations, animations and interactive media were constructed for this study. This research study involved three evaluation steps (see Figure 1). First, the survey was pilot-tested with one personal injury lawyer experienced in using medical illustrations and animations for demonstrative evidence in the courtroom and at mediation. Based on feedback from this interview, the survey questions and corresponding visuals were modified. The revised survey was then presented to a group of medical illustrators and their feedback was incorporated into the final survey. The resulting survey was used in formal interviews with the sample population. PHASE 1: CREATION OF THE HYPOTHETICAL CASE A cervical fracture dislocation injury was chosen because this injury may result in permanent damage to the spinal cord with significant functional day-to-day sequelae for the injured person, and may have other associated bony and soft tissue injuries (Raisman 1995). The number of these injury issues permitted the creation of several visuals with different characteristics. This injury was also chosen because more than 10,000 Americans (National Library of Medicine 2002) and about 1,050 Canadians (The Canadian Paraplegic Association 2000) suffer spinal cord injuries each year, making it a major cause of legal actions. Characteristics of the injury depicted in this study include fracturing of the spine, disruption of soft tissues that support the spine, dislocation of the spinal configuration, misalignment of the zygapophyseal (facet) joints into a jump facet position, and permanent damage to the spinal cord with resulting incomplete quadriplegia that allows the client only minimal use of the upper arms. A condensed summary for the hypothetical client, called John Doe, was written for the study. The details of the injury were compiled from a composite of six similar cases illustrated for clients of Artery Studios Inc (a Toronto-based studio specializing in medical-legal visuals) during the past five years. PHASE 2: PRODUCTION OF ILLUSTRATIONS Radiographs, medical reports and photographs were compiled. Existing illustrations were analyzed, and several new illustrations were created in Adobe Photoshop™ (version 7.0), based on x-rays, computed tomography (CT) scans and magnetic resonance imaging (MRI) scans. The final illustrations included a side view of the fractured cervical spine; a longitudinal sectional view through the damaged spinal cord; insets of the facet joint injury; an orientation illustration; depictions of the surgical stabilization of the spine; depictions of long-term complications, including urinary and bowel management, loss of innervation issues, and urinary tract infections; and views of potential future development of syringomyelia. All images to be included in the exhibits were electronically assembled in Adobe PageMaker™ (version 6.5). A base layout that incorporated a lateral x-ray, an orientation illustration, and a large illustration of the fractured and dislocated spine was assembled with titles, labels, leader lines and other graphic elements (see Figure 4, Panel A). Recognized visual communication techniques (visual cues), including color features such as coding and saturation, contrast, spatial relationships, magnification, graphic devices such as arrows, cut-away views of anatomical structures, multiple views of a structure, and the inclusion of labels and leader lines (Wilson-Pauwels 1997; Gloeckner 1987) were incorporated. Implied movement, size and position of images, and layout of the text with pictures (Goldsmith 1987) were also taken into consideration. Multiple versions of layouts and illustrations were created using these theories of design (see Figures 4 –13). All panels were printed as full-color images (10” x 15”) on white matte paper, mounted on stiff black boards and assembled into a display portfolio with appropriate labels. PHASE 3: PRODUCTION OF ANIMATIONS Mechanism of injury animation A digital model of the cervical spine was created with Cinema 4D™ (version 8.5) and BodyPaint 3D™ (version 2). The model was animated to show forward hyperflexion and other details of the injury mechanism, and composited in Adobe After Effects™ (version 6.0). Animated trauma x-ray An animation was created depicting the proposed mechanism of fracturing of the cervical spine as if the injury were occurring while being viewed on an x-ray machine. An x-ray of the injured cervical spine was scanned and imported into Photoshop™. Line drawings depicting the cervical spine in stages of injury – from a normal appearance to the final fracture dislocation – were created, imported into Photoshop™ and converted to a golden color to contrast with the x-ray. Photoshop™ was used to add masks and make adjustments. The Photoshop™ file was imported into After Effects™ and animated. PHASE 4: PRODUCTION OF INTERACTIVE MEDIA Virtual model of the injured spine Cinema 4D™ and BodyPaint 3D™were used to create digital models of the skull and injured cervical spine based on information from the trauma x-rays. A QuickTime™ virtual reality (QTVR™) model was then rendered. The interactivity of the visual was intended to allow the participant to move the model in virtual space - namely, to rotate and zoom in on it. Transitional Flash™ slider A lateral view x-ray showing the initial fracture dislocation of the cervical spine and a corresponding full-color illustration of it were scanned and imported in Flash™ MX (version 7.2). The two images were programmed so that the user could transition between them (i.e., so that the x-ray gradually dissolves into the rendered illustration and vise versa). The position of a slider button was linked to changes in the amount of transparency between the images. This type of demonstrative aid was originally created by the faculty and students in the Biomedical Communications program at the University of Toronto to enable verification of the accuracy of medical-legal illustrations based on radiographic images (Lax et al 2004a; Lax et al 2004b). Step-by-step animation Color illustrations of the hypothetical surgical stabilization of the fracture dislocation injury were rendered in Photoshop™. Text and graphics were added and composited with the illustrations. JPEG versions of each frame were placed as individual slides into Microsoft PowerPoint™, and formatted with QuickTime™ cross-fade transitions between each slide. PHASE 5: DESIGN OF PARTICIPANT PROFILE QUESTIONNAIRE A pre-interview questionnaire was designed to collect demographic information about the study participants: for example, the number of years of practice in personal injury litigation, experience using demonstrative evidence and computer proficiency. PHASE 6: RECRUITMENT OF PARTICIPANTS A sample of 21 experienced lawyers who had used medical-legal illustrations or animations during mediation or trial between 1992 and 2004 was selected from the client list of Artery Studios. Because of the large size of the studio's practice, these lawyers comprised the majority of lawyers who regularly use customized medical-legal visuals in Southern Ontario. One lawyer agreed to participate in pilot testing, and 20 lawyers agreed to participate in 90-minute individual in-person interviews, which were held in the participants’ offices. A briefing package was sent to each lawyer. This contained a letter reiterating the details of the study, an informed consent form for the interview, the hypothetical case outline, and the pre-interview questionnaire, to be completed in advance and collected at the time of the interview. PHASE 7: DESIGN OF SURVEY QUESTIONNAIRE Development of the questionnaire The questionnaire was designed according to guidelines of Salant and Dillman (1994). Open-ended questions were included to increase feedback (Salant and Dillman 1994; Dillman 2000) and to allow each lawyer to express his or her opinions fully. Questions were asked to probe lawyers’ perceptions about which characteristics made a particular visual helpful: clarity, credibility, effectiveness, ease of use, persuasiveness, admissibility and impact. Page layouts in the portfolio displayed versions of each visual being tested. Closed-ended questions were asked about which variation of the visual aids lawyers preferred, and open-ended questions were asked about the lawyers’ opinions about the effectiveness of the images. Additional questions that elicited feedback about admissibility and other legal issues, and the strategy of using visuals for personal injury litigation, were also formulated. Pilot testing: formative evaluation of the survey One lawyer who had been practicing personal injury litigation for nine years and had experience using both medical illustrations and animation was selected to pilot test the survey. This litigator's experience was representative of the participant population. A structured interview was conducted with this lawyer to identify any potentially confusing issues in the survey (including those in the pre-interview package) to determine the relevance of the survey questions and to obtain any other reactions. The survey artwork and questions were modified, based upon this formative feedback (see Figure 1). The modified survey was then presented to three medical illustrators, each of whom had over 18 years of experience in the field. Feedback from this formative evaluation was also incorporated into the study (see Figure 1). PHASE 8: EXECUTION OF SURVEY Interviews: formal evaluation Twenty lawyers were interviewed during the month of November 2004. All interviews were audio recorded and notes were taken in case there were any problems with the recording. The length of each interview was noted. Data analysis Answers to the pre-interview questionnaire were tallied and graphed with Microsoft Excel™. All 20 taped interviews were transcribed. The responses were then grouped into three categories: general demonstrative evidence or legal issues, illustration, and motion media. An Excel™ spreadsheet was created to summarize and track the answers both quantitatively and qualitatively. Responses were analyzed for recurrent themes. Similar answers from 60% or more of the respondents were considered conclusive responses and used to formulate the final list of recommended guidelines for the creation of visuals for demonstrative evidence. Results STUDY POPULATION All 20 participants in the survey were white; 3 were women. Participants had considerable experience in personal injury litigation: 60% (12/20) of the lawyers had practiced for more than 20 years. Respondents used numerous formats of demonstrative evidence in their practice (Figure 2); over 66% (12/18) used demonstrative evidence in more than 50 cases (Figure 3). All participants had used illustrations during mediation, 75% (15/20) had used large customized medical illustration panels and 45% (9/20) had used animations. Sixty-five percent (13/20) of respondents reported being quite comfortable using computers. Of the 18 lawyers who used computers regularly, 12 (67%) used PowerPoint™ to present their cases. ILLUSTRATIONS Radiographic images When shown the panels that contained or omitted a scan of the x-ray from which the trauma illustration was rendered (Figure 4), 100% (20/20) of the lawyers preferred Panel A with the x-ray. Most (90%, 18/20) said that inclusion of the x-ray added credibility, with many noting that it reinforced that the illustration was accurate. And while CT and MRI scans were not depicted in Figure 4, all (100%, 20/20) believed that their inclusion, where relevant, would have the same effect. Orientation illustration All (100%, 20/20) participants preferred a panel that included an orientation illustration showing the location of the injured spine in the neck of the hypothetical client (Figure 5); 85% (17/20) said that this clarified the information presented. When shown orientation illustrations of the injured cervical spine in the context of the human form, rendered either realistically or generically (see Figure 6), 100% (20/20) preferred the realistic rendering; 95% (19/20) thought this treatment helped to personalize the depiction of the injury to their client. When lawyers were shown the panels in Figure 7, 60% (12/20) of the participants preferred the orientation illustration rendered without skin tone (Panel A). They thought that the spinal anatomy stood out better. Of the 40% (8/20) who preferred the image with the skin tone, 50% (4/8) thought that the skin color added an element of realism. Labels All (100%, 20/20) lawyers thought that the name of the client should be included on the panel. Seventy-five percent (15/20) said that the name helped to personalize the illustration to their plaintiff. Preferences for labels of about 4, 8 and 18 words taken directly from the medical reports were evaluated, with 94% (18/19) preferring labels with several (8 or more) words in the description. Of the 20 participants, 15 (75%) preferred the use of labels that incorporated medical terminology rather than lay terms. Ten (66%) of these 15 respondents volunteered that their medical experts would explain the technical terms during the trial. Amount of information on panels About three-quarters (74%, 14/19) of participants preferred that a larger panel composed of six images (Figure 8) be split into two separate panels. The majority (68%, 13/19) thought that this treatment would be less likely to overwhelm the viewer. Focal point of rendering Most (95%, 19/20) participants preferred an illustration of the injured cervical spine in full saturation (Figure 9, Panel A) to that of a rendering that focused on the area of injury (Figure 9, Panel B). Of these respondents, 63% (12/19) disliked Panel B, commenting that it looked “distorted” and “artsy,” and 53% (10/19) said that they may have admissibility or other concerns with this style of image because it placed too much emphasis on the area of injury. Illustrations of normal anatomy, surgery and injury complication issues Almost two-thirds (65%, 13/20) of participants preferred the inclusion of a normal comparator illustration that contrasted with the injury depiction on the panel (Figure 10). Of the 35% (7/20) who thought this illustration was not necessary for this case, 57% (4/7) said they would want a normal illustration for other types of cases. Three-quarters (75%, 15/20) of participants thought that a panel depicting surgical stabilization of the spine (Figure 11) should be included in the demonstrative evidence dossier. Of these 15, 87% (13) said that it would increase understanding of what the client had gone through. Out of the 20 respondents, 17 (85%) said that illustrations depicting long-term complications of the injury (e.g., Figure 12) would be very important to include in a case like this. Seventy-five percent (15/20) said that they would be important tools for settlement meetings and 80% (16/20), responded that they would be important for trial. When shown a panel depicting possible future spinal cord deterioration (Figure 13), 95% (19/20) of participants said that it should be included in the demonstrative evidence: 70% (14/20) said it was extremely or very important and 25% (5/20) said it was important.
Animation of the mechanism of injury Most respondents said that an animation depicting the proposed mechanism of injury (Figure 14) would help them educate the viewer about the topic: 85% (17/20) during mediation, and 95% (19/20) during a trial. Only 15% (3/20) said they would not use the animation during mediation, but would use it to educate the jury if the case went to trial. Animated trauma x-ray Most participants thought that the animation showing the proposed spinal injury mechanism as if it were viewed on an x-ray machine (see Figure 15) would be an effective visual: 80% (16/20) thought it would be effective for use during mediation and 85% (17/20), at trial. However, 85% (17/20) had concerns with its admissibility: 7 (41%) of these 17 were concerned about depicting details of the injury mechanism when the exact mechanism may not be completely understood.
Interactive 3D model The ability to move the QTVR™ interactive model (Figure 16) demonstrating the details of the injured spine in virtual space was well received: 85% (17/20) of participants expressed a strong liking for it and believed it would be admissible, and 80% (16/20) thought that they or their medical experts would be readily able to use the interactivity of the visual. However, 25% (5/20) volunteered that the jury might have a problem using it. Transitional Flash™ slider The immediate response from 75%, (15/20) of respondents to the Flash™ slider that transitioned between the trauma x-ray of the injured spine and the corresponding illustration (Figure 17) was that it added credibility to the medical illustration and that it would assist with admissibility issues. However, after using the slider for a few moments, 50% (10/20) of respondents questioned what use they would make of it, 60% (12/20) thought that there might be problems with admissibility because of its limited utility, and 40% (8/20) wondered whether the court would perceive this type of visual as “gimmicky”, “too slick” or unnecessary. Step-by-step slide animation Most participants thought that a step-by-step animation depicting the surgical stabilization of the fractured spine (Figure 18) would be effective: 75% (15/20), during mediation; 80% (16/20), at trial. About half of those who liked the visual thought that their medical expert could better explain the details of the surgery using a detailed presentation such as this rather than panels. Seventy percent (14/20) preferred this style of presentation to the panel format.
Some participants discussed the issue of voice-overs after viewing the injury mechanism animation. Feedback indicated that voice-overs are not admissible in Canadian courts, but 25% of the participants (5/20) were interested in having them in animations for mediation. Many lawyers were willing to take more chances during settlement negotiations. The majority (60%, 12/20) said they would use intimidation tactics on a difficult file that they wanted to settle, rather than proceeding to trial, and half (50%, 10/20) of the lawyers said they would want the visuals to be more graphic or dramatic in such circumstances. Although the study asked questions on visuals depicting the case of a cervical fracture dislocation, participants often extrapolated to other cases in answering probing questions. Discussion Medical-legal visuals must be simple and focused, and clarify the issues (Turbak et al 1994). This study’s participants echoed this assertion. The plaintiff lawyers in this study stressed that the visuals should be credible and admissible; maximize understanding; depict the entire injury sequence, including mechanism of injury, trauma, surgery and complications; and be personalized to the specific plaintiff. Interest was expressed in interactive user-controlled media. This study used a survey population of 20 lawyers. The participants were believed to be generally representative of their peers. They were from towns and cities of varying sizes: 10% (2/20) practiced in towns with a population of less than 100,000; 65% (13/20), in cities with a population between 100,000 and 500,000; and 25% (5/20), in metropolitan Toronto with a population of over 2.4 million (Brinkhoff 2003). The results may, however, have a regional bias because the study population was restricted to lawyers practicing in Southern Ontario. The consumer-spending index in Ontario is 11% higher than that of the average Canadian expenditure per household, and the unemployment rate is 6.6%, just below the national average of 6.8% (Statistics Canada 2004). Results may have varied if testing had been performed in different socioeconomic regions of the country. Because of the familiarity of the participants with the use of medical-legal illustrations or animations, the participant lawyers may have been biased in favor of the types of visuals that they are accustomed to using. However, their extensive expertise gave them the knowledge required to assess the qualities of effective medical-legal visuals for mediation or trial, and was the fundamental reason for selecting them for the study. Respondents may also have been predisposed to the style of the visuals since they were used to receiving visuals created by Artery Studios. However, the responses provided during interviews were sometimes contrary to previous or usual feedback, which suggested that they were open to new concepts and able to respond objectively to questions asked. Not stratifying results by the participants’ level of experience may also have introduced a bias – it may have obscured the influence of experience on participants’ judgments and preferences for certain types of visuals. Interestingly, although the study used visuals depicting only the case of a cervical fracture dislocation, participants often extrapolated to other types of cases in answering probing questions. As a result, the proposed guidelines may be valid for other similar cases. Analysis of the results of this study suggests the following guidelines for creating medical-legal illustrations for plaintiff personal injury litigation:
These guidelines were compiled from conclusive themes, namely, from opinions expressed by at least 60% of the respondents. Each lawyer, of course, would have a unique approach to arguing a file. Therefore, when creating medical-legal visuals, the medical illustrator should ask lawyers about their preferences to ensure the compatibility of the images with each lawyer’s style of litigation. Further research in the field of medical-legal visualization might investigate issues such as the effect of color, variations on new technologies, differences between American and Canadian preferences for visuals for litigation, issues of admissibility, use of visuals in different geographic or socioeconomic communities, perception of different graphic elements and evaluating visuals for cases that involve other types of injuries. All of these issues might also be investigated with lawyers from the defense bar to see if there are significant differences in approach to the visuals they use. Positive feedback was expressed to the interactive media presented in this survey. Some lawyers cautioned that for such demonstrative evidence to be used, the case law might have to change. Medical illustrators creating medical-legal visuals using new media may need to testify more often to increase the admissibility of presentations that use innovative technology. Medical-legal illustrators may have to play a larger role to set precedents for the admission of visuals. The recommended guidelines derived from this study should help medical illustrators in the field of medical-legal visualization produce more effective exhibits, and better satisfy the needs of personal injury plaintiff lawyers. References: Babcock, C.L., and Bloom, J.S. 2001. Getting your message across: Visual aids and demonstrative exhibits in the courtroom. Litigation 27(3):41-44. Beck, J.M. 1984. A medical illustrator’s guide to the production of demonstrative evidence. Master’s thesis. The University of Texas Health Science Center, Dallas. Brinkhoff, T. 2003. http://www.citypopulation.de/Canada-Ontario.html (accessed Mar 06). The Canadian Paraplegic Association. 2000. Spinal cord injury in Canada. Diamond, S.S. 1997. Illuminations and shadows from jury simulations.
Law and Dillman, D.A. 2000. Mail and internet surveys: The tailored design method.
New Diner, J. 1963. Medical illustration in the court of law. The Journal of the Association of Medical Illustrators 14:21-23. Douglas, K.S., Lyon, D.R., and Ogloff, J.R.P. 1997. The impact of graphic photographic evidence on mock jurors decisions in a murder trial: probative or prejudicial? Law and Human Behavior 21(5):485-501. Feigenson, N., and Dunn, M.A. 2003. New visual technologies in court: Directions for research. Law and Human Behavior 27(1):109-126. Gloeckner, P.L.A. 1987. A semiotic analysis of medical illustration. Master’s thesis. The University of Texas Health Science Center, Dallas. Goldsmith, E. 1987. The analysis of illustration in theory and practice. In: Houghton, H.A., and Willows, D.M. ed. The Psychology of Illustration, Vol 2. New York: Springer Verlag. Irwin, D. 1987. Medical illustration as demonstrative evidence. The Advocates’ Society Journal 6(4):39-40. Jew, R., and Peterson, M.Q. 1995. Envisioning persuasion: Painting the picture for the jury. Trial October: 76-82. Joye, M.C. 2000. Avoiding 10 pitfalls of demonstrative evidence. Trial November: 94-101. Kassin, S.M., and Dunn, M.A. 1997. Computer-animated displays and the
jury: Lax, L., Taylor, I., Wilson-Pauwels, L., and Scardamalia, M. Dynamic
Curriculum Lax, L., Rogers, T., Brierley, M., Wilson-Pauwels, L., and Mackay, M. Mader, S.R. 1995. The preparation of customized medical illustration
exhibits for McLeish, J.A. 2004. Preparing for Trial. In: The Oatley-McLeish Guide
to Personal National Library of Medicine, Medline Plus. Spinal cord injury. http://www.nlm.nih.gov/medlineplus/tutorials/spinalcordinjury/htm/_no Oatley, R.G. 2000. Addressing the jury: Achieving fair verdicts in personal
injury Oatley, R.G. 2004. The strategic use of demonstrative evidence at trial. In: The Oatley-McLeish Guide to Personal Injury Practice in Motor Vehicle Cases. Aurora, Canada: Canada Law Book Inc. Oatley, R.G. 2004 and McLeish, J.A. 2004. Demonstrative evidence. In: The Oatley-McLeish Guide to Personal Injury Practice in Motor Vehicle Cases. Aurora, Canada: Canada Law Book Inc. Oliver, G. 1994. Medical art in the courtroom. Journal of Audiovisual Media in Medicine 17:12-14. Raisman, G. 1995. Stroke and spinal injury. National Institute for Medical Research. http://www.nimr.mrc.ac.uk/millhillessays/1995/spinjury.htm (accessed Jan 05). Salant, P. and Dillman, D.A. 1994. How to conduct your own survey. New York: John Wiley & Sons Inc. Simmons, R., and Lounsbery, J.D. 1994. Admissibility of computer-animated reenactments in federal courts. Trial September: 79-82. Statistics Canada. 2004. http://www.statscan.ca (accessed Mar 06). Turbak, N.J., Bailey, W.S., Heninger, S.D., Rosen, W.W., and Christy, G. 1994. If a picture’s worth a thousand words… Trial September: 62-71. Wheatley, B.H. 2004. A mediator's view of the best approach to private mediation. In: The Oatley-McLeish Guide to Personal Injury Practice in Motor Vehicle Cases. Aurora, Canada: Canada Law Book Inc. Wilson-Pauwels, L. 1997. Bringing it into focus: Visual cues and their role in directing attention. The Journal of Biocommunication 24(3):12-16. Worthen, B.R., and Sanders, J.R. 1987. Educational Evaluation: Alternative Approaches and Practical Guidelines. New York: Longman. Stephen R. Mader, B.Sc., B.Sc.AAM, M.Sc.BMC, CMI Linda A. Wilson-Pauwels, A.O.C.A., B.Sc.AAM, M.Ed.,
Ed.D., CMI Sharon L. Nancekivell, B.A., B.Ed., M.A. Leila R. Lax, B.A., B.Sc.AAM, M.Ed., Ph.D.(c), CMI Anne M.R. Agur, B.Sc.O.T., M.Sc., Ph.D. David M. Mazierski, B.Sc.AAM Many thanks to the following people for their assistance on this research project and paper: Kate Billingsley, Jennifer Bosy, Peter Caldwell, Janice Chan, Kathryn
Chorney, Lima Colati, Susan Hall, Marlene Herbst, Dino Pulera, Julie Saunders,
Thanks also to Sue Seif for her review and editing of an earlier draft of this paper. Programming for the transitional Flash™ slider interface was designed for the medical-legal context by Jodie Jenkinson: Assistant Professor, Biomedical Communications, Institute of Communication and Culture, University of Toronto at Mississauga; and Associate Member, Institute of Medical Science, Faculty of Medicine, University of Toronto This paper was been rewritten from a Master’s Research Paper submitted
for the degree of Master of Science in Biomedical Communications from
the University of Toronto (2005).
|
Copyright 2005, The Journal of Biocommunication, All Rights Reserved