Julie Saunders, BA, MScBMC, Ralph Z. Stern, MD, MHSc, FRCP(C), Linda Wilson-Pauwels, AOCA, BScAAM, MEd, EdD, Nicholas Woolridge, BFA, BScBMC, MSc
To increase awareness of migraine diagnosis criteria among health professionals, we developed a prototype physician–patient interview video on DVD. Design methodology involved a needs assessment, two editing models (commentary interspersed vs. contiguous), and an evaluation with medical students, residents and primary care physicians. This evaluation assessed user preferences for the two editing models, and provided qualitative feedback for future development. Results established that respondents preferred the interspersed audio commentary over commentary appearing at the end of the video.

Figure 1. Storyboards developed from script for physician–patient interview.
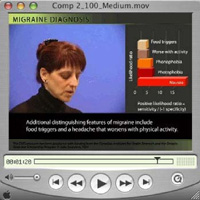
Figure 2. Beta design of project, modeled on CablePulse24 television news channel layout.

Figure 3. Two streams of information: audio commentary and onscreen text summary.

Figure 4 (a) (Model A, above). Editing model for commentary interspersed throughout video.
Figure 4 (b) (Model B, below). Editing model for commentary following video. |
Introduction
Video is an important media form in medical education. It is used to present taped lectures (Cronin et al. 1994); model techniques for emulation (Bashman & Treadwell 1995, Lundevall et al. 1994); and for feedback and self-evaluation (Premi 1991; Beckman & Frankel 1994; Edwards et al. 1996; Chou & Lee 2002).
Video on its own is an important learning tool, and has been demonstrated to be even more effective when combined with other verbal modes of learning (Bashman & Treadwell 1995). A meta-study (Pan & Cornell 2002) on the optimum use of video in educational programs formulated a number of recommendations, such as using video in combination with text or narration, and using video for the purpose of illustration, simulation, and modeling. However, the study did not provide editing guidelines on how to integrate video material with instructional material. A thorough search of the literature did not reveal any studies that outlined editing methods and evaluated their effectiveness in medical education.
This study evaluates user satisfaction with two different editing methods of combining video material and a didactic audio commentary in a DVD format. Physicians’ need to recognize and accurately diagnose migraines provided an appropriate subject matter for the study.
Migraine
Migraine is a complex disorder that is difficult to diagnose and treat. Population-based studies have shown that approximately 5% of men and 15% to 17% of women suffer from migraine attacks (Pryse-Phillips et al. 1997). Despite its common occurrence, the disorder is under recognized, under diagnosed, and under treated (Pryse-Phillips et al. 1997).
Poor physician–patient communication is the most frequently cited barrier in the diagnosis and treatment of migraine (Pryse-Phillips 2002). The typical physician–patient interview, lasting only five to eight minutes, does not provide enough time for patients to adequately describe their symptoms and disabilities (Pryse-Phillips 2002). Additionally, physicians tend to provide information to their patients, rather than engaging in a shared process of ‘building’ a history with them (Pryse-Phillips 2002).
The difficulty of understanding migraine and the importance of good communication in its diagnosis and treatment makes the topic a suitable area for a continuing medical education (CME) course for family physicians. Our project targeted these needs through the creation of a video of a simulated physician–patient interview that includes an audio commentary by Dr. Ralph Kern (a neurologist at Toronto’s Mount Sinai Hospital) about current findings in the field of migraine research.
Development of the Prototype DVD
This project was divided into three stages: 1) Needs assessment to determine primary care physicians’ knowledge of headache and preferences for media delivery, 2) Content development and editing, 3) Evaluation of the video by medical students and family practice residents, and 4) Field testing among a group of primary care physicians participating in an acute migraine treatment study.
Development Stage 1: Needs assessment
Methods
We constructed a questionnaire to determine primary care physicians’ preferences for the delivery of CME on headache disorders (Kern et al. 2005). Questions on the use of media in CME were designed according to Mamary and Charles (2003). Questions on the diagnostic guidelines for migraine were modeled from Pryse-Phillips et al. (1997). Questions on communication skills training were modeled from Purdy (2002).
Dr. Ralph Kern conducted the needs assessment with 650 primary-care physicians from Canada, France, Japan, Spain, UK, and USA (Kern et al. 2005). Results showed that primary-care physicians’ current self-reported knowledge of headache is generally inadequate. Many physicians are not interested in headache-specific CME activities. As a result, we determined that a CME course on this topic would need to be presented in an engaging format to stimulate interest.
Development Stage 2: Content development
Methods
Script
We chose a complex case from Rapoport et al. (1999) as the basis for the video script. Using this model, a history was constructed for a woman in her 30s with a stressful lifestyle that contributed to her migraines, and who had been previously misdiagnosed with tension headache.
The structure of the interview dialogue was based on the model of ‘building’ a history, as opposed to ‘taking’ one, as presented in Haidet and Paterniti (2003). Their approach emphasizes two-way information sharing, as demonstrated in their scripted example of a skilled interview, which served as a model for questions, pacing and phrasing.
Video
We began video production with storyboards (Figure 1) that outlined the planned shots, props, and costumes.
The videotape was made at the University of Toronto (U of T) Surgical Skills Centre at Mount Sinai Hospital, Toronto, using a Canon XL1S Digital Video Camcorder (Canon USA Inc. 2002.), a standard three-point lighting kit, lavaliere microphones, a television monitor, two actors, a camera operator, and two assistants. Set-up, tests and taping of the seven-minute script took four hours. To ensure enough high-quality recordings for editing, we taped three takes of each shot (Schoonover et al. 1983).
The general structure of the edited video follows the D.W. Griffith formula for editing (Donald & Spann 2000), beginning with a long shot that establishes the scene, cutting in to a medium shot as the action begins, and finally using close-ups for heightened drama. The color cast of the video was corrected with filters in Final Cut Pro HD™ (Apple Computer Inc. 2004.). Ambient noise in the audio track was eliminated with Sound Soap™ 1.1.1 (Berkley Integrated Audio Software Inc. 2004.) and audio levels were normalized in Peak 3 DV™ 3.21 (Berkley Integrated Audio Software Inc. 2002.).
Audio commentary
The audio commentary, written and recorded by Dr. Ralph Kern and Julie Saunders (edited in Sound Soap and Peak), addressed significant aspects of the physician-patient interview and introduced topics in current migraine research.
Creation of two editing methods for evaluation
In developing two editing methods for integrating video and didactic audio commentary, we examined various media sources, such as television news and teaching videos.
Many television news channels, such as CablePulse24 (a local Toronto news station), convey multiple streams of information simultaneously through video and onscreen text. Beta testing of the multiple streams of information model (Figure 2) with graduate students indicated that it was difficult to follow all of the information presented. As both the video interview and the audio commentary were important for teaching about migraine diagnosis, we chose to not use this format.
Videos designed for teaching purposes, such as one produced to teach nurses communication techniques (Concept Media 1990), have often used a model of presenting a simulated real-life scenario, with pauses for audio commentary and an onscreen text summary to reinforce essential information. We decided to model our project on this format so that there would be no competition between the two streams of information (Figure 3).
Two different strategies were designed to test the pairing of the video with the commentary. The first model broke the interview into discrete chunks, followed by relevant audio commentary (Figure 4a). The audio commentary was reinforced with short onscreen text summaries. The second model presented the interview in its entirety, followed by all of the audio commentary (Figure 4b).
Hypotheses
With model A, we hypothesized that the interspersed expert commentary would be easier to follow because it is broken into small chunks, however the constant interruption of the interview video would be disorienting.
With model B, we hypothesized that the uninterrupted narrative would be more coherent and enjoyable, however, the contiguous chunk of expert commentary at the end of the program would present the user with a quantity of information that might be difficult to absorb.
Despite these competing advantages and disadvantages, the research team hypothesized that participants would prefer Model A over Model B.
Stage 3: Summative Evaluation
Methods
Approval for the research protocol was secured from the Ethics Review Office at U of T. The questionnaire, including qualitative and open-ended questions, was designed to evaluate user experience with educational video and DVD, user interest in migraine education, and user satisfaction with editing methods and media delivery.
Three target audiences participated in the evaluation: second-year medical students, residents, and primary care physicians participating in an acute migraine treatment study. Second-year medical students at U of T were contacted through their e-mail listserv. Three students took part in the evaluation. Each student participated in a one-hour individual session in a Biomedical Communications conference room viewing the two editing models, answering a written questionnaire, and participating in a debriefing session.
Seventeen family physician residents at Mount Sinai Hospital in Toronto also participated in the evaluation. The evaluation was conducted as part of a lecture session with Dr. Ralph Kern. The residents listened to a 40-minute lecture on migraine diagnosis, spent 20 minutes viewing the two editing models, and then filled out the questionnaire during the last 30 minutes of the lecture.
Dr. Ralph Kern conducted an evaluation with 21 primary care physicians at the ZAP Second Annual Investigator Meeting in Lisbon, Portugal, in September 2004.
Results
Two out of the three medical students preferred the audio commentary interspersed throughout the video. The students who preferred this version felt that it was easier to absorb the didactic information because it was broken down into chunks, as reflected in the following comment:
“The one with it interspersed was more preferable. It allowed for some contextual relevance to the facts being narrated. Furthermore because it came in brief periods the information was not too overwhelming.”
During our debriefing session, one of the students clarified that while most of the audio commentary was highly relevant to diagnostic features demonstrated in the interview, some of the audio commentary, which was related more to general principles, could have been more appropriately placed as either an introduction to the video or as a conclusion for the video.
Fourteen of the 17 residents preferred the interspersed audio commentary. Comments included:
“Interest level was maintained and important learning points were reinforced before too much information was presented.”
“Commentary discusses/explains points in history taking; more prompt and relevant at that point in time; easier to digest.”
When asked what other content they would like to see included on a DVD about migraine, five of the 14 residents were especially interested in migraine treatment information (Table 1).
Table 1. Residents’ responses for additional features/content for the DVD resource
Number of Responses |
Response |
5 |
Treatment/management information |
3 |
Printed component |
1 |
Pathophysiology and prescriptions |
1 |
Questions at the end for review |
1 |
Comparison of different types of headache similar to migraine but not migraine |
1 |
Red flags that would help distinguish worrisome headaches vs. migraine |
1 |
Examples of how a patient will initially present |
1 |
Patient resource |
Seventeen of the 21 primary care physicians preferred the interspersed audio commentary. They felt that this version provided interest, facilitated learning, and was a helpful format for teaching their students:
“The physician may induce discussion as the case goes on and then hear what the expert has to say.”
“I would use the interruptions to do more discussion from the audience.”
Two of the three medical students, 10 of the 17 residents, and 12 of the 21 primary care physicians stated that the DVD program had increased their interest in migraine diagnosis.
Of the seven primary care physicians who suggested other content for inclusion on a DVD about migraine, four were interested in diagnostic material (Table 2).
Table 2. Primary care physicians’ responses for additional features/content for the DVD resource
Number of Responses |
Response |
4 |
Diagnostic information |
2 |
Treatment information |
1 |
More complex material |
Table 3 outlines an analysis of all comments from both the medical students’ and the residents’ questionnaires, revealing that there are a number of additional features they would like to see included in the DVD program. The most frequent suggestions related to supplementing information delivery by narration or print, with seven requests for a print-out of the commentary, and four requests for a narrated or printed version of the International Headache Society (IHS) criteria for diagnosis. Suggestions for additional DVD interactivity included four requests for scene selection, one request for a pop-up menu of topics, and one request for a more interactive experience.
Table 3. Medical students’ and residents’ responses for desired DVD content delivery methods
Number of Responses |
Response |
7 |
Print-out of commentary |
4 |
IHS criteria presented more slowly with narration, or in printed form |
4 |
Scene selection |
2 |
More information on references |
2 |
Review questions |
1 |
Pop-up menu option of additional topics relevant to sections in the interview |
1 |
More interactivity |
Table 4 outlines an analysis of comments from the primary care physicians’ questionnaires, revealing that there are a number of extra features that they would like to see included in the DVD delivery of the program. Like the residents and students, they were interested in increasing the value of the expert commentary and the IHS criteria, by accompanying them with written text, by presenting the information more slowly, or by creating a separate section for text-based material (i.e. slides). Unlike the residents and students, they had no suggestions for DVD navigation, although one primary care physician was interested in greater interactivity for text-based slides.
Table 4. Primary care physicians’ responses for desired DVD content delivery methods
Number of Responses |
Response |
2 |
Separate section for slides |
1 |
IHS criteria presented more slowly |
1 |
More written information on screen |
1 |
More cases |
1 |
French version |
1 |
Slides more interactive |
Discussion
We created two models of editing that we judged to be equally valid. The surprisingly strong response from all three participant groups in favor of Model A (the interspersed audio commentary) proved that evaluation was justified.
This study has a number of limitations. The evaluations were not conducted under ideal conditions, or with ideal instruments. The sample group of three medical students was too small for statistical analysis. Had the evaluation with the medical students been conducted during the school year, rather than during the summer, it is likely that the participation rate would have been higher. Even so, the hour-long, one-on-one interviews with the medical students provided a wealth of qualitative data.
The evaluation conditions with the residents were also not ideal. Because the evaluation was conducted in a classroom setting, all residents viewed Model A and B together. This may have influenced their preference for the first version, as they may have become bored watching the same content a second time. Splitting the audience into two groups and reversing the order of presentation would have strengthened the validity of the research.
Finally, the evaluation of primary care physicians involved in an acute migraine treatment study is a biased sample of individuals who have a strong intellectual and working interest in headache disorders and may not be representative of primary care physicians in general.
The Migraine Diagnosis video can be viewed at http://www.painm2c.ca/Pub/Pub_Front.asp.
Click on the link for videos (at the far right).
Conclusion
We have created a simulated physician–patient interview and audio commentary that an audience of medical students, residents and primary care physicians perceived as a motivator to learn more about migraine.
Participants’ comments clearly indicate that additional content items and DVD delivery features would make the DVD a more complete resource for migraine diagnosis.
A number of suggestions for DVD delivery have already been incorporated: a menu for scene selection by commentary topic; separate expanded and narrated movies of the International Headache Society criteria for migraine diagnosis; and a user-controlled text-based slideshow of all audio commentary references, with brief synopses of study methodology and research.
DVD navigation and interactivity in an educational program is an important area of study especially for educators who are deciding on a format for programmatic delivery. Qualitative feedback on user satisfaction as well as quantitative data on learning efficacy are needed to assess DVD’s potential as an educational medium.
Acknowledgments
Dr. Michael Salter, MD, PhD, Director, University of Toronto Centre for the Study of Pain and Professor, Department of Physiology, Faculty of Medicine
Professor Sharon Nancekivell, BA, BEd, MA, Biomedical Communications, Institute of Communication and Culture, U of T at Mississauga
Professor Kelly Brine, Bmath, Biomedical Communications, Institute of Communication and Culture, U of T at Mississauga
Ms. Lisa Satterthwaite RPN/OR, U of T Surgical Skills Centre, Mount Sinai Hospital, Toronto
Cast and crew of the video shoot: Shelley Wall, Vivian Moens, Teddy Cameron, Gloria Situ, Nicholas Woolridge
Dr. Gary Shapero, Markham Headache Centre, Markham Ontario.
AstraZeneca Inc.
This study was funded in part by the Canadian Institute for Health Research and the Ontario Graduate Scholarship program.
References
Apple Computer Inc. 2004. Final Cut Pro HD. California, USA: Apple Computer, Inc.
Bashman, J.G., and T.W. Treadwell. 1995. Assessing the effectiveness of a psychodrama training video. Journal of Group Psychotherapy, Psychodrama & Sociometry 48(2):61-69.
Beckman, H.B., and R.M. Frankel. 1994. The use of videotape in internal medicine training. Journal of General Internal Medicine 9(9):517-521.
Berkley Integrated Audio Software Inc. 2002. Peak 3 DV 3.21. California, USA: Berkley Integrated Audio Software Inc.
Berkley Integrated Audio Software Inc. 2004. Sound Soap 1.1.1. California, USA: Berkley Integrated Audio Software Inc.
Canon U.S.A. Inc. 2002. Canon XL1S Digital Video Camcorder. New York, USA: Canon U.S.A. Inc.
Chou, C., and K. Lee. 2002. Improving Residents' Interviewing Skills by Group Videotape Review. Academic medicine 77(7):744.
Concept Media. 1990. Techniques of therapeutic communication. Irvine: Concept media, Inc.
Cronin, M.W., G.L. Grice, and R.K. Olsen, Jr. 1994. The effects of interactive video instruction in coping with speech fright. Communication Education 43(1):42-53.
Donald, R., and T. Spann. 2000. Fundamentals of Television Production. Iowa: Iowa State University Press.
Edwards, A., A. Tzelepis, C. Klingbeil, T. Melgar, M. Speece, H. Schubiner, and R. Burack. 1996. Fifteen years of a videotape review program for internal medicine and medicine-pediatrics residents. Academic Medicine 71(7):744-748.
Haidet, P., and D. Paterniti. 2003. "Building" a history rather than "taking" one: a perspective on information sharing during the medical interview. Archives of Internal Medicine 163(10):1134-1140.
Kern, R., G. Shapero, G. Boudreau, P. Squire, and J. Dawes. 2005. There is a strong unmet need for improved headache education among primary care physicians: results from a primary care needs assessment. Headache Care 2(1): 47-49.
Lundevall, S., I. Njølstad, and I. Aaraas. 1994. Stop the video and involve the observers: an inter-reflective method to stimulate doctors' learning about their own consultations with patients. Medical Teacher 16(2/3):189-195.
Mamary, E. and P. Charles. 2003. Promoting self-directed learning for continuing medical education. Medical Teacher 25(2):188-190.
Pan, S. And R. Cornell. 2002. Optimum use of video in light of cognitive learning theories. Journal of Educational Media & Library Sciences 40(2):156-169.
Premi, J. 1991. An assessment of 15 years experience in using videotape review in a family practice residency. Academic Medicine 66(1):56-57.
Pryse-Phillips, W. 2002. Evaluating migraine disability: the headache impact test instrument in context. The Canadian Journal of Neurological Sciences 29 (suppl2):S11-S15.
Pryse-Phillips, W., Dodick, D., and Edmeads, J. 1997. Guidelines for the diagnosis and management of migraine in clinical practice. CMAJ 156:(9)1273-1287.
Purdy, R.A. 2002. Migraine: the doctor-patient link. Results of a needs assessment. The Canadian Journal of Neurological Sciences 29 (suppl2):S3-S7.
Rapoport, A.M., F.D. Sheftell, and R.A. Purdy. 1999. Advanced therapy of headache. Hamilton: B.C. Decker Inc.
Schoonover, S.C., E.L. Bassuk, R. Smith, and D. Gaskill. 1983. The use of videotape programs to teach interpersonal skills. Journal of Medical Education 58(10):804-810.
Authors
Julie Saunders, BA, MScBMC, Graduate, Biomedical Communications, Institute of Communications and Culture, U of T at Mississauga
Ralph Z. Kern, MD, MHSc, FRCP(C), Division of Neurology, Mount Sinai Hospital, Toronto, Department of Medicine, U of T
Linda Wilson-Pauwels, AOCA, BScAAM, MEd, EdD, Biomedical Communications, Institute of Communication and Culture, U of T at Mississauga
Nicholas Woolridge, BFA, BScBMC, MSc, Biomedical Communications, Institute of Communication and Culture, U of T at Mississauga
Julie Saunders, MScBMC, graduated from the Biomedical Communications program at the University of Toronto at Mississauga in 2004. She currently works as an Illustrator/Animator at Artery Studios in Toronto, producing medical-legal illustrations and animations. She is also an instructor in digital image manipulation at the Art Institute of Toronto.
Email: julie.saunders@toronto.ca
|
