|
|
|
Bridging the Gap: A Web-based Visual Database of Medications to Address the Cognitive Needs of Patients and the Information Needs of Patients and Their Health Care Providers |
| Linda Wilson-Pauwels, AOCA, B.Sc.AAM,
M.Ed., Ed.D.
|
AbstractMulti-drug regimens present many challenges to patients, especially to senior patients. This case study explores the communications difficulties and medication compliance difficulties experienced by a 90-year-old patient who suffered two heart attacks, and the resulting development of a visually-based medication organizer, PharmaPlanner, by researchers at the University of Toronto. The project included development of two Web-based applications, one to author a comprehensive database of vector-generated icons of prescription medications in Canada, and the other to assist pharmacists in the field construct custom, visual, drug-regimen organizers for clients. Project researchers tailored visual material for the cognitive abilities of the target patient population, ensuring that the maintainability, reusability, expandability and sustainability of the applications and data followed industry-standard, object-oriented design techniques. Target audience evaluation of visual material is employed to ensure effective design of the PharmaPlanner icons, menus, and interface. The Drug Identification Number (DIN), a unique identifier of drug forms and dosages, emerged as a crucial element in ensuring that prescriptions and their visual representations are accurately matched. Case StudyTwo and a half years ago, 90-year-old Alice Smith (not the patient’s real name) suffered a major heart attack and was taken to the local hospital by ambulance. One week later she returned home with a new 12-medication regimen; it was soon obvious to her daughter that she needed help organizing her medications. Her daughter noticed that Alice consistently referred to the drugs on her regimen by their appearance: “the little yellow pill,” “the big red pill.” This inspired her daughter to create a visual medication list from the information found on the two-page summaries of each drug supplied by Alice’s pharmacist. The list included the name of the drug and the preferred time of day to take the medication, and, most importantly, a color-coded picture of each tablet or pill. The list was revised to group the medications according to the time of day that they were to be taken. The sorts of problems faced by Alice and her physicians are alarmingly common, and their impact is far from trivial. An aging population means that more and more people will be on complex multi-drug regimens (also known as polypharmacy). While an aging populace is perhaps the primary target for the development of better management tools, many other conditions, such as HIV infection, kidney failure, and immunosuppressive therapy require the patient to manage a complex regimen of drugs. An estimated 33 percent of avoidable, medication-related hospital admissions are attributed to drug compliance failures (McDonald, 2002). Patients with multiple physicians (for instance: a general practitioner, a cardiologist, and a rheumatologist), may end up with duplicate or incompatible medications; maintaining current knowledge of a patient’s prescriptions is an administrative burden for physicians. Alice’s visual menu is known as a medication adherence aid (MAA), and it was the basis for the development of PharmaMenu. The difficulties faced by Alice’s medical personnel in accessing her current prescriptions provided the impetus for developing PharmaPlanner, a network-accessible database of a patient’s drug regimen. IntroductionA multidisciplinary research team (visual communicators, pharmacists, computer programmers and educators) at the University of Toronto is designing PharmaPlanner, a multi-modal computerized database system. System development was based on the needs assessments of patients, caregivers, and health care providers and through an iterative process of formative evaluation, with insight from the domains of adult education, visual communication, and the medication-taking practices of patients with chronic illnesses.The design of PharmaPlanner has been informed by four key premises: “Beeping pillboxes and talking wristwatches may seem to be the stuff of science fiction, but more and more elderly patients are relying on such devices to make sure that they adhere to their increasingly complex medication regimens” (McGarry Logue, 2002). Age-associated cognitive decline adds to the challenge of recalling medication regimens (Park et al. 1999). Research has shown that pictorial aids are particularly effective in enhancing information recall in elderly subjects (Winograd et al., 1982; Roedder-John and Cole, 1986) and in patients with low literacy skills (Houts, et al. 2001). Patients, their family members, and often health care providers are already creating organization tools and memory aids that consist of lists, both handwritten and electronically generated. Most of these MAAs are missing the essential component, the visual representation of the medication and the dynamically driven organization function. Also, many have not been developed based on systematically described patient needs, nor have they been comprehensively evaluated (Lee, 2004). PharmaPlanner addresses our four key premises with the following two components:
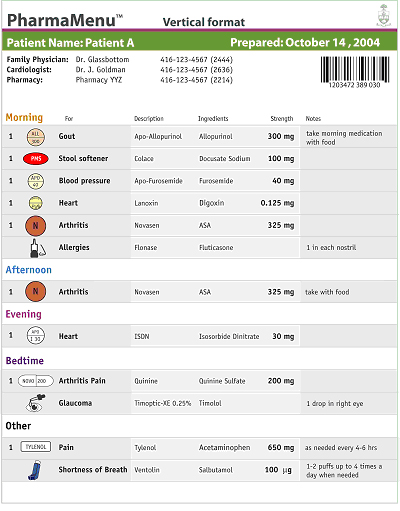
While placing great emphasis upon the visual appearance of medication, PharmaPlanner’s
PharmaMenu provides associated textual information about a patient’s
medication regimen, such as medication names, indications, and dosages.
Medications are grouped according to the time of day at which they are taken
(morning, afternoon, evening, bedtime, or other). The PharmaMenu is dynamically
generated, readily updatable, printable in color, and resolution independent.
It is also potentially electronically accessible to all health care providers
and patient caregivers who have been authorized by the patient to access
the password-protected database. BackgroundBecause primary care physicians write approximately 80 percent of prescriptions for people 65 years of age or older (Tamblyn et al., 1996), effective interventions to optimize prescribing in primary care are a priority (Tamblyn et al., 2003). One third of preventable hospital admissions for adverse drug reactions were associated with patient noncompliance (McDonnell & Jacobs, 2002). “It is up to providers to simplify medication regimens for elderly patients, that could enhance treatment adherence and obviate the dangers of adverse reactions, drug-drug interactions, and medication errors” (McGarry Logue, 2002). The ultimate outcome would be an improved quality of life. Terrence Montague in Patients First 2004 writes, “… education of and communication between provider and patient are implicated in resolving the problem of poor compliance with therapy. It is not just a patient issue.” One of the conditions proposed as a strategy to reduce medication errors is availability of patient information at the point of use (Naylor, 2002). This is consistent with health care provider and patient experiences that suggest that patient-specific medication information is not easily accessible to those individuals within the system who help patients (especially vulnerable patients such as seniors) with their medications. Somerville and Phillips (2003) wrote, “Various hospital departments including pharmacy services must address many complicated issues regarding appropriate education prior to discharge to assure proper medication compliance. Poor discharge instructions about a patient’s new medication regimen can lead to serious consequences.” There is a lack of consistent access to current and comprehensive information about the patient’s medications by family physicians, specialists, family members, pharmacists, nurses, and home-care providers. This places the senior at unnecessary risk for drug-related errors. What would have happened if Alice had entered the hospital and her Emergency Medicine Physician had access to a well organized visually enhanced drug regimen online? He would have been better informed, and far more likely to make a rapid assessment of her condition. Access to her drug regimen would have also facilitated the integration of new medications.A database-driven retrieval system, accessible to the patient, family, and health care providers, could improve the coordination of the various lay and professional caregivers who are helping seniors with their medication-taking practices and save the amount of time that the family physician spends communicating this information to all specialists. Tamblyn et al. (2003) write, “Primary care physicians provided only half of all medical services to their elderly patients, who, on average, received prescriptions from at least 3 other physicians and filled those prescriptions at several pharmacies.” Numerous MAAs have been developed to help patients understand how, and remember when, to take their medications. One of the most popular MAAs with seniors is the dossette. The obvious problem with this type of MAA is that once the pills are removed from the labeled dispenser and compartmentalized within the dossette, the patient may not remember the medication’s intended purpose. The color, shape, and size of the drug then become the language of communication. What would happen if Alice had a PharmaPlanner that accompanied her dossette? She would then be able to identify each of the medications and why she is taking them.Electronically generated reminder charts or medication organizers have been used in a variety of settings to help improve patient compliance (Raynor et al., 1993). Our literature review identified only one group in the United States that has, in a limited capacity, incorporated visual aids and technology to create a medication organizer for transplant patients (Somerville and Phillips, 2003). This tool is enhanced by approximately 250 scanned, resolution-dependent photographs of medications, in a standalone application available within a single institution. The PharmaPlanner system, described here, has been created on a more advanced platform that ensures maintainability and expandability. Vector-based medication icons and menus are generated dynamically from a database and drug metadata is drawn from the Health Canada Drug Product Database, ensuring sustainability and wide access to up-to-date customizable information. Our review also uncovered several photographic databases of drug appearance. All of the photographic databases suffered from one or more of the following flaws: they were proprietary to a particular manufacturer or software vendor (especially in the pharmacy-management software space); they were not to scale; they were incomplete; there was poor or inconsistent quality control of the photographic capture; or they were not tied to a reputable, unique identifier to distinguish drug forms and dosages from one another. In addition, all photographic representations suffer from ambiguity when representing pill and tablet features that are difficult to resolve photographically, such as debossed text, but which are essential to medication recognition. For this reason we elected to represent the medications as vector-generated line drawings. This paper addresses the design methodology of PharmaPlanner and how the program will help to bridge the medication communication gap between patients and their health care providers. Hypothesis and Objectives of the PharmaPlanner ToolWe hypothesize that a well-designed drug regimen management program could reduce patients’ medication-related complications, reduce medication errors, and enhance communication between patients and their health care providers. Specific objectives in the development of PharmaPlanner are to:
Design MethodologyOur research has shown that continual creation of up-to-date medication menus for patients is a very complex problem. With a view to simplifying this process for all stakeholders, PharmaPlanner has been designed to facilitate reusability, expandability, multiple platform implementation, and general sustainability. Description of the ToolsThe PharmaPlanner system consists of two core components or Web applications:
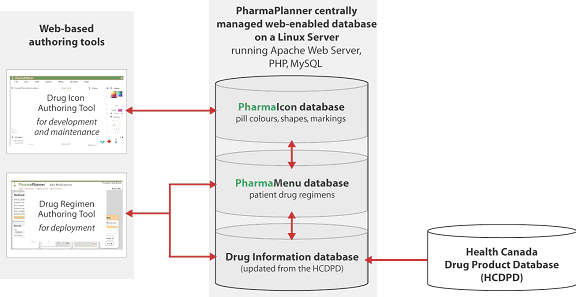
Both of the above tools function as Web applications authored in Macromedia Flash MX 2004 (Macromedia Inc., 1993-2004). These components adhere to standard graphical user interface guidelines for desktop applications (Apple Computer, 1992). The applications open within a Web browser and link to a centrally managed, Web-enabled database. This allows multiple copies of an application to be distributed to different platforms simultaneously at minimal cost, with real-time data sharing over the Internet. New users can learn how to use the interface quickly, leveraging existing computing experience with ordinary desktop applications. Since the applications reside on the central server, improvements can be implemented on-the-fly without the need to update individual copies of the software (Figure 1). Program ArchitectureGenerally speaking, the PharmaPlanner system design adheres to the principles of object-oriented programming. Objects are divided into:
In PharmaPlanner, both Transaction and Interface Objects exist within the Flash interface, and these communicate with Data Objects programmed in PHP (The PHP Group, 2001-2004) that access icon and drug regimen information in a MySQL (MySQL AB, 2004) database. Data ArchitectureAs indicated in Figure 1, when PharmaPlanner team members want to create
or modify a drug appearance record (PharmaIcon), they access the Drug
Icon Authoring Tool through a secure Web interface. Changes they make
are stored in a MySQL database running on a central server; PHP scripts,
also running on the central server, act as a bridge between the Flash
interface and the database. Unique drug IDs are maintained by use of the
Drug Identification Number (DIN), which is regularly updated from the
publicly accessible Drug Product Database on Health Canada’s servers
in Ottawa.
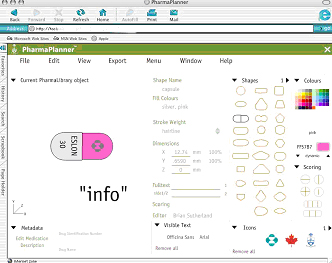
Figure 1 - PharmaPlanner Database Architecture PharmaPlanner references the Drug Product Database, a central registry of drug products approved for use in Canada, which is maintained by the Therapeutic Products Directorate of Health Canada. It contains approximately 23,000 medications, of which approximately 5,000 are relevant to this study, as they are self-administered prescription and over-the-counter medications (the remaining ~18,000 entries include vitamins, cosmetics, homeopathic remedies, and veterinary drugs). Each individual product in the Health Canada Drug Product Database has an identifier called the Drug Identification Number (DIN) that is unique for every dosage and form of the drug available. The DIN is a key link between the medication icons and the associated descriptive textual information or metadata available about the product. Referencing open standards in drug identification ensures that this system can take advantage of other public data services as they are created, and this practice ensures that the system’s resources will be compatible with many other applications also used to manage the medication use chain. PharmaPlanner Drug Icon Authoring ToolThe PharmaIcon library is the first documented vector-generated visual database of standardized medications in use in Canada. For flexibility, clarity and accuracy of color, this tool renders the appearance of the medication (size, color, shape, scoring pattern, etc.) from a string of parameters and drug description metadata referencing standard drug vector prototypes (Figure 2). The non-pill medications, such as inhalers, drops, patches, etc., also reference original prototype icons in vector format. The icons are generated in association with the corresponding DIN and output from the Drug Icon Authoring Tool as a text string. This mode of production provides the greatest flexibility to tailor the visual appearance of the medication icons for the intended audience. For instance, a geriatric audience might prefer a heavier stroke weight, larger type size and color adjustments. Changes to these visual features can be made database-wide, as our evaluations allow us to find the best way to represent the drugs visually. The ability to access the PharmaPlanner Drug Icon
Authoring Tool over the Internet, with full edit trails, means that
the PharmaIcons could be authored in many places before they are approved,
ensuring that the PharmaIcon objects accurately reflect the medications
available to communities of practice.
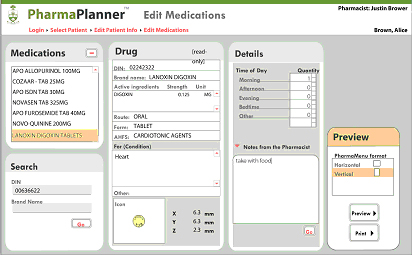
Figure 2. PharmaPlanner Drug Icon Authoring Tool PharmaPlanner Drug Regimen Authoring ToolTo generate patient medication regimen menus, a second Flash application was designed as a data input system for pharmacists (Figure 3). The pharmacist inputs the patient’s drug regimen as well as pertinent patient information and contact information for the prescribing physicians. PharmaIcon data is retrieved alongside the Health Canada Drug Product Database data, including drug chemical name and trade/brand name and dosage. The pharmacist then inputs the patient’s medication dosage schedule, as well as other pertinent information to define a menu, which is then saved to the MySQL relational database. Lastly, the pharmacist selects output preferences and generates a “PharmaMenu” that can be viewed in a print or electronic format.
Figure 3. PharmaPlanner data input screen
Figure 4. A hypothetical
PharmaMenu (vertical format)
Preliminary EvaluationsDuring the past two years, we have conducted both informal and formal evaluations of the PharmaPlanner menu design with members of the target audience. These early pilot evaluations have helped to develop protocols for more extensive evaluations of visual material (icons, symbols and interface design). The evaluations also have highlighted the importance of the DIN as the link to compiling text and visual mediation information in Canada. Future evaluations will be conducted through semi-structured interviews to understand the needs of the various targeted audiences: patients in complex “burdensome” care who are on a large number of drugs, physicians who care for the elderly, pharmacists who generate lists and use them to teach patients about their medications, and homecare nurses who require information at the point of care. Future ResearchThe research team is presently conducting Phase I of the evaluation of
the PharmaPlanner program at the Sunnybrook Health Sciences Center’s
Dialysis Unit, Toronto, Ontario. This evaluation phase includes preliminary
program evaluation and assessment of icons, symbols, and the PharmaPlanner
interface. The data will contribute to establishment of best practice
guidelines for the design of tools that help patients with their medication-taking
practices. As well, we expect that it will contribute to our understanding
of the important function served by visual aids in facilitating communication
between patients and their health care providers. It also will provide
new potential data for patient utilization of the Canadian provincial/federal
electronic medical record system and design of medication information
tools that can be incorporated into these systems. EpilogueDue to ailing health, Alice decided to move into a seniors' residence a week after her heart attack. The nurse in the residence immediately telephoned Alice's family physician for a list of her medications, which was an essential step in determining whether Alice was well enough to be accepted into the residence, as it was not a chronic care facility. Alice continues to use the menu prepared and regularly updated by her daughter. Her health care providers now ask her how they can obtain PharmaMenus for their other patients. ReferencesApple Computer Inc. 1992. Macintosh Human Interface Guidelines. Menlo Park, CA: Addison-Wesley Publishing Company.Health Canada. Toward Electronic Health Records. Office of Health and the Information Highway. Health Canada. January 2001. http://www.hc-sc.gc.ca/ohih-bsi/pubs/2001_ehr_dse/ehr_dse_e.html#Electronic Center for Drug Evaluation and Research. 2004. Drugs@FDA. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm Accessed on Dec. 10, 2004. Lee, B., J. Bajcar, and L. Wilson-Pauwels. 2004. A review of the current literature on the design and evaluation of medication adherence aids. (abstract R24). Canadian Pharmaceutical Journal 137(5):24. Houts, P.S., J.T. Witmer, H.E. Egeth, M.J. Loscalzo, and J.R. Zabora. 2001. Using pictographs to enhance recall of spoken medical instructions II. Patient Education and Counseling 43:231-242. Macromedia, Inc. 1993-2004. Macromedia Flash MX 2004. San Francisco, CA. http://macromedia.com/ McDonnell, P., and M.R. Jacobs. 2002. Hospital admissions resulting from preventable adverse drug reactions. The Annals of Pharmacotherapy 36:1331-6. McGarry Logue, R. 2002. Self-medication and the elderly: how technology can help. American Journal of Nursing 102(7):51-55. Merriam, S.B., and R.S. Caffarella. 1999. Learning in Adulthood. San Francisco, CA: Jossey-Bass Inc. Montague, T. 2004. Patients First: closing the health-care gap in Canada. John Wiley & Sons Canada Ltd. (pg. 62). MySQL AB. 2004. MySQL 4.0. Uppsala, Sweden. http://dev.mysql.com/ McDonnell, P.K., and M.R. Jacobs. 2002 Hospital admissions resulting from preventable adverse drug reactions. The Annals of Pharmacotherapy 36:1331-6. Naylor, R. 2002. Medication errors: Lessons for education and healthcare. Radcliff Medical Press: Oxon, UK. Park, D., R. Morrell, and K. Shifren. Processing of medical information in aging patients. Lawrence Erlbaum Associates, Publishers: Mahwah, NJ. The PHP Group. 2001-2004. PHP 4.1. http://www.php.net/ Raynor, D., T.G. Booth, and A. Blenkinsopp. 1993. Effect of computer generated reminder charts on patients’ compliance with drug regimens. British Medical Journal 306:1158-1161. Roedder-John D., and C.A. Cole. 1986. Age differences in information processing: Understanding deficits in young and elderly consumers. The Journal of Consumer Research 13(3):297-315. Somerville K.T., and K. Phillips. 2003. The MedPlanner: An internet-based dynamic medication education tool. Advances in Pharmacy 1(2):112-120. Tamblyn R., A. Huang, R. Perreault, A. Jacques, D. Roy, J. Hanley, P. McLeod, and R. Laprise. 2003. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. Canadian Medical Association Journal 169(6):549-556. Tamblyn R.M., P.J. McLeod, M. Abrahamowicz, and R. Laprise. 1996. Do too many cooks spoil the broth? Multiple physician involvement in medial management and inappropriate prescribing in the elderly. Canadian Medical Association Journal 154:1177-84. Walsh S. 2004. The clinician’s perspective on electronic health records and how they can affect patient care. British Medical Journal. 328:1184-7. Winkelman W, and K. Leaonard. 2004. Overcoming structural constrains to patient utilization of electronic medical records: A critical review and proposal for an evaluation framework. Journal of the American Medical Informatics Association 11(2):151-161. Winograd E., A. Smith, and E. Simon. 1982. Aging and the picture superiority effect in recall. Journal of Gerontology 37:70-75. AcknowledgementsThis research is supported by a grant from Merck Frosst Canada Inc. and the Bell University Laboratories Health Communications Lab in the Faculty of Medicine at the University of Toronto.This research is supported by a grant from Merck Frosst Canada Inc. and the Bell University Laboratories Health Communications Lab in the Faculty of Medicine at the University of Toronto. Authors:Linda Wilson-Pauwels, AOCA, B.Sc.AAM, M.Ed., Ed.D., is Director of Biomedical Communications (BMC), Institute of Communication and Culture, University of Toronto at Mississauga (UTM) and Director of the Master of Science in Biomedical Communications (MScBMC) program, Institute of Medical Science, Faculty of Medicine, University of Toronto (UofT). Dr. Wilson-Pauwels is a tenured Professor in BMC and is cross-appointed to the Department of Surgery. She is a visual communicator with advanced degrees in higher education. Her interest is in information transfer to target audiences, development of visual organizational tools, and visual cues and their role in directing attention. Jana Bajcar, B.Sc.Phm., M.Sc.Phm, Ed.D., FCSHP, is an Associate Professor in the Leslie Dan Faculty of Pharmacy & Department of Family and Community Medicine, Faculty of Medicine at UofT. She is an academic pharmacist with a doctoral degree in health education. Her research deals with reduction of preventable medication-related problems through innovations in patient and clinician medication education. Jodie Jenkinson, B.A., M.Sc.BMC, is an Assistant Professor specializing in instructional design in BMC. She is the author and designer of The Prostate Centre, a CD-ROM and Web site and co-author of the BreastMatters Web site, both educational programs designed for patients of The University Health Network in Toronto. Jenkinson has a cross-appointment to the Department of Surgery. Her research is in interface design and data visualization. Brian Sutherland, B.A., M.Ed., is an Instructional Technology Analyst and multimedia/database programmer with the Academic Computing Group of the Ontario Institute for Studies in Education, U of T. Applied projects include national database-hypermedia and CD-ROMs for Manulife Financial and learning objects recognized by the National Council of Teachers of Mathematics. Nicholas Woolridge, B.F.A., B.Sc.AAM, M.Sc., is a tenured Associate Professor specializing in animation and multimedia in BMC. He is the co-author of Anatomy 300/303 Interactive Lab Companion, a hybrid Web/CD-ROM program. Woolridge has a cross-appointment to the Department of Surgery. His expertise is in medical visualization, hypermedia, and database design. Meaghan Brierley, B.F.A., PGDip Medical Photography, M.Sc.BMC, is a Research Associate with the IVIS (Interpretive Visualization) Group and an instructional media designer and developer with the Bell University Lab in Health Communication, Faculty of Medicine, U of T. Linda Wilson-Pauwels, Jodie Jenkinson, Nicholas Woolridge, and Meaghan Brierley are founding members of the IVIS Group http://www.bmc.med.utoronto.ca/ivis/ in Biomedical Communications. Correspondence: l.wilson.pauwels@utoronto.ca |
Copyright 2004, The Journal of Biocommunication, All Rights Reserved